Best Gynecologist Clinic in Gurgaon

July 10, 2026
Understanding PCOS: A Common Concern for Indian Women
Polycystic Ovary Syndrome, commonly known as PCOS, is one of the most frequently diagnosed hormonal disorders affecting women of reproductive age today. In India, the prevalence of PCOS ranges from 3.7 to 22.5 per cent, depending on the population studied and the diagnostic criteria used. A 2024 ICMR national multicentric study found a weighted prevalence of 19.6% among Indian women. This means nearly one in five women of reproductive age in our country is affected by this condition.
First described by Doctors Stein and Leventhal in 1935, PCOS encompasses a syndrome of polycystic ovaries accompanied by systemic symptoms affecting reproductive, metabolic, and psychological health. While the name suggests the presence of ovarian cysts, it is important to understand that PCOS is fundamentally a hormonal imbalance, the ovaries produce higher-than-usual levels of androgens (male hormones), which disrupts ovulation and the menstrual cycle.
The condition typically presents between the late teens and early thirties, often first noticed when a woman tries to conceive. However, PCOS does not discriminate, it can affect adolescents and postmenopausal women as well.
The Link Between PCOS and Infertility: What You Need to Know
The connection between PCOS and infertility is one of the most concerning aspects for women diagnosed with this condition. It is important to address the question directly: PCOS is the single most common hormonal cause of infertility in Indian women. Studies indicate that 70–80% of women with PCOS experience infertility.
But here is what every woman should understand, PCOS-related infertility is also one of the most treatable forms of infertility.
Why Does PCOS Affect Fertility?
Conception depends on a predictable sequence: a follicle matures, an egg is released (ovulation), it meets sperm in the fallopian tube, and the resulting embryo implants in the uterine lining. PCOS disrupts the first two steps.
The underlying mechanism involves:
- Excess Androgens: Elevated levels of male hormones prevent follicles from maturing normally
- Insulin Resistance: Many women with PCOS have reduced sensitivity to insulin, resulting in hyperinsulinaemia, which further increases androgen production
- Hormonal Imbalance: Raised luteinising hormone (LH) levels from the anterior pituitary affect normal ovarian function
Many small follicles develop in the ovaries, but none release an egg. Without ovulation, there is no egg for sperm to fertilise. This is why women with PCOS often experience long cycles (35+ days), skipped periods, or months of unpredictable bleeding.
The Reassuring Truth
Despite these challenges, PCOS rarely affects egg quality, the uterus, or the fallopian tubes. The ovaries typically hold an above-average reserve of eggs. The problem is almost entirely one of release timing and release timing is the most treatable variable in fertility medicine.
Once ovulation is restored, pregnancy outcomes for women with PCOS are comparable to those of women without the condition.
Symptoms of PCOS: Recognizing the Signs
PCOS manifests through a variety of symptoms that can affect physical health, emotional well-being, and quality of life. Common symptoms include
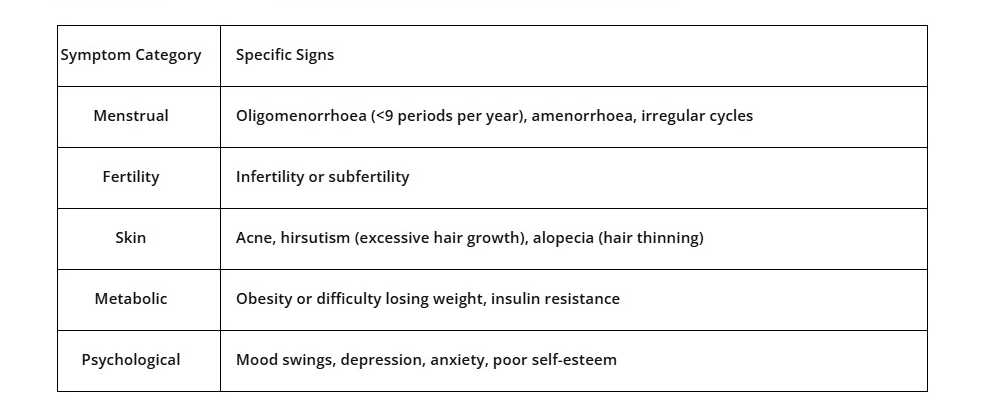
A study conducted in Northeast India found that among women with PCOS, clinical hyperandrogenism manifested as acne (49.05%), hirsutism (43.39%), and alopecia (28.3%). Menstrual issues involved oligomenorrhea (45.28%), amenorrhea (30.18%), and dysmenorrhea (33.96%).
If you are experiencing any combination of these symptoms, it is essential to consult a qualified obstetrician or gynecologist for proper evaluation.
Diagnosis: How PCOS Is Identified
PCOS is diagnosed based on the Rotterdam criteria (2003), which require the presence of at least two of the following three features:
- Oligo-ovulation or anovulation (irregular or absent ovulation)
- Clinical and/or biochemical signs of hyperandrogenism (excess male hormones)
- Polycystic ovaries on ultrasound
It is worth noting that polycystic ovaries on ultrasound are very common and can be seen in up to 33% of women of reproductive age. However, the majority of women with polycystic ovaries do not have features of PCOS and do not require intervention.
Early diagnosis is crucial, not just for fertility concerns, but because PCOS is associated with increased risk of type II diabetes, cardiovascular disease, and metabolic syndrome.
Treatment and Management: Your Path Forward
The good news is that PCOS is manageable, and with the right approach, most women with PCOS can conceive and have healthy pregnancies. Fertility specialists approach PCOS using a graduated treatment ladder:
Step 1: Lifestyle Optimization (First 3–6 Months)
For women with a BMI above 25, a modest weight loss of 5–10% alone restores ovulation in 30–50% of cases. This is not about aggressive dieting, it is about reducing insulin resistance, the metabolic engine behind most PCOS.
A structured plan should include:
- Guidance from a qualified dietitian
- Consistent sleep routine
- Combination of resistance training and cardio
- Stress reduction techniques
Even normal-weight women with PCOS benefit from insulin-sensitising nutrition patterns.
Step 2: Medical Ovulation Induction
If lifestyle changes alone are not sufficient, ovulation induction medications such as letrozole or clomiphene citrate are often the first line of medical management.
Step 3: Assisted Reproductive Techniques
For women who do not conceive with ovulation induction, options include Intrauterine Insemination (IUI) or In Vitro Fertilization (IVF).
Step 4: Advanced Interventions
In some cases, procedures such as transvaginal ovarian drilling prior to IVF may improve outcomes. Emerging research also explores combination therapies, including the use of ethinylestradiol-cyproterone acetate with raloxifene, which has shown effectiveness in managing PCOS-associated infertility.
Pregnancy with PCOS: What to Expect
Women with PCOS who conceive require specialised care during pregnancy. PCOS is associated with increased risk of:
- Gestational diabetes mellitus (GDM)
- Gestational hypertension
- Preeclampsia
- Preterm rupture of membranes
A study found that among pregnancies conceived after infertility treatment, PCOS was the most common female cause (56.7%), with medical complications including gestational hypertension (26.7%) and GDM (26.7%).
However, with meticulous monitoring and evidence-based care, women with PCOS can have successful pregnancies and healthy outcomes.
When to See a Doctor
You should consult an obstetrician or gynecologist if you experience:
- Irregular or absent menstrual periods
- Difficulty conceiving after trying for 6–12 months
- Signs of excess hair growth, acne, or hair thinning
- Unexplained weight gain or difficulty losing weight
- A family history of PCOS or related conditions
Early intervention makes a significant difference. The diagnostic gap remains the single biggest obstacle to getting pregnant with PCOS, not the condition itself.
Conclusion: Hope and Help Are Available
PCOS and infertility are closely linked, but this is not a reason to lose hope. PCOS is one of the most treatable causes of infertility, and with the right medical guidance, lifestyle modifications, and treatment plan, most women with PCOS can achieve their dream of motherhood.
At Dr. Shweta Wazir’s practice, we provide compassionate, evidence-based care tailored to each woman’s unique needs. Whether you are seeking a diagnosis, exploring fertility options, or managing PCOS during pregnancy, we are here to guide you every step of the way.
📞 Contact Us
Dr. Shweta Wazir
Obstetrician & Gynecologist
📱 +91 84481 28007
🌐 www.drshwetawazir.com
Serving women across India with dignity, expertise, and care.
Leave A Comment